AN INTRODUCTION TO CREATINE
Many profits in the supplement industry are generated by making exaggerated claims about their products. Despite the popularity of such supplements, few are very well researched and the industry itself isn’t well regulated. In fact, one popular pre-workout stimulant, Jack3d, was recently banned in the United States because it contained an illegal dietary supplement, dimethylamylamine (DMAA), that has been linked with the development of cardiovascular problems.
Creatine, however, is a popular supplement used for increasing muscle development and athletic performance that has been well-researched and has been consistently proven to produce these effects. Its effects can be explained by basic biochemical principles. This article will also touch on the ethics regarding supplementation.
Creatine, derived from the Greek word for flesh, (kreas), was first discovered in 1832, when Michel Eugene Chevreul extracted the compound from meat. Its anabolic effects would be confirmed in humans in the early 20th century when it was found that supplementation increased creatine content in muscles. Supplementation didn’t become mainstream until the 1990s when two Olympic gold-medallists credited creatine as part of their success. By 1996, an estimated 80% of athletes at the Atlanta Olympics were using creatine too. The significance of creatine supplementation and the subsequent increase in muscle and athletic performance must first be prefaced with an introduction to some general metabolic concepts.
Biochemistry of Creatine
Creatine is used to regenerate adenosine triphosphate (ATP), the “universal currency of the cell”. Many metabolic processes in the body, such as the ones involved in sprinting and weightlifting, have energy requirements. Essentially, ATP is the money that employees, the chemical reactions, are compensated with. When the employees don’t get paid, they won’t do work; similarly, if there isn’t any ATP, the chemical reactions involved in muscle contraction won’t occur.
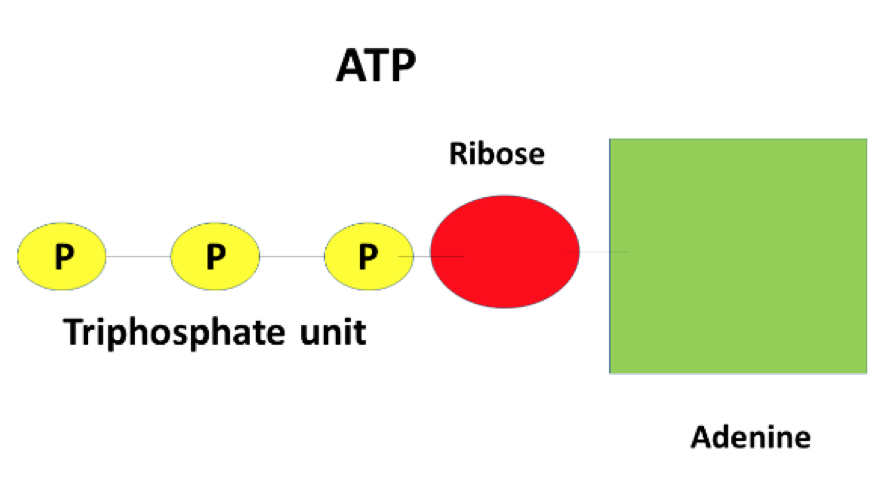
ATPs unique capacity as a vehicle for energy transfer can be explained by its molecular structure. ATP is a molecule consisting of an adenine, ribose, and most importantly, a triphosphate unit. The bonds between the phosphate groups store large amounts of energy and are what makes ATP so effective. When a chemical reaction demands it, one phosphate bond is cleaved in ATP and energy is released, driving the chemical reaction to proceed.
The reaction can be represented chemically as:
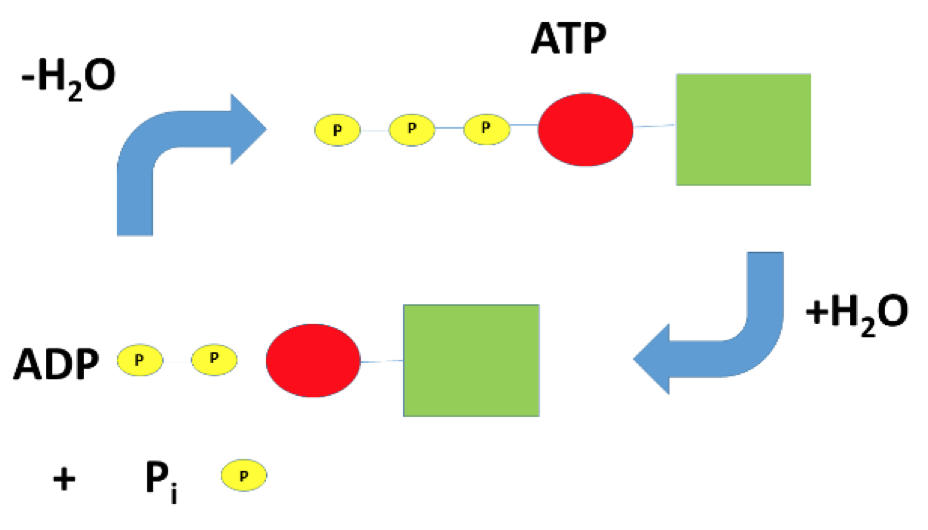
ATP + H2O < -> ADP + Pi + energy
The < -> symbol indicates that this reaction can occur in two directions and is dependant on the amounts of each of the components in the reaction. A simplified explanation of the concept is that the forward reaction (ATP + H2O -> ADP + Pi + energy) occurs when energy is needed, and the backwards reaction (ADP + Pi + energy -> ATP + H2O) occurs when the amount of ATP is low.
Hydrolysis, the insertion of water into ATP, causes the release of three components: adenosine diphosphate (ADP), which is ATP without one phosphate group, inorganic phosphate (Pi), the one phosphate group that is released during the reaction, and energy, which is utilized by the cell. Conversely, the chemical synthesis of ATP from ADP and Pi is condensation, the removal of water. ATP is generated by various metabolic processes in the mitochondria and is used at various sites throughout the cell.
Chemical reactions can be placed into two categories: those that need an input of energy and those that don’t. A real-world analogy is that it’s the difference between walking up the stairs and riding an elevator to the top floor of an apartment building. Using an elevator is no hassle, but hiking up the stairs does require work much like a chemical reaction that requires an input of energy. So where does this energy to hike up the stairs come from? The food that’s been eaten throughout the day. What food does for hiking up the stairs is what ATP does for causing chemical reactions to occur.
With all this said, it would make sense for the body to have massive reservoirs of ATP; however, this isn’t the case. In reality, skeletal muscle only stores enough ATP to power a couple seconds worth of high-intensity exercise. As a result, ATP needs to be either replaced or resynthesized on an ongoing basis in muscle. Creatine can replenish these stores of ATP, and that is the basis for why it is used as a supplement.
Creatine can be phosphorylated in a similar way to ADP. The process is mediated by an enzyme called creatine kinase. The enzyme generates creatine phosphate from ATP in the mitochondria, making phosphocreatine and ADP. Since ATP is limited in the cell, creatine acts as a holder for high-energy phosphate groups similar to a bank account. After transfer, ADP stimulates further metabolic processes and the generation of more ATP. Creatine phosphate, however, migrates to muscle fibres. As ADP is generated from muscle contraction, creatine phosphate regenerates ATP allowing for further contraction according to the following reaction:
phosphocreatine + ADP + H+ < -> ATP + creatine
The dephosphorylated creatine then returns to the mitochondria to be rephosphorylated. It should be noted that this reaction, like the previous one, is a reversible process indicated by the double-headed reaction arrow, < ->. The reverse reaction occurs in the mitochondria, and the forward reaction occurs at sites which mediate muscle contraction.
Creatine is naturally occurring compound that is largely synthesized in the liver at about 1g/day, however 95% of it is found in skeletal muscle. It is also obtained from diet, primarily from meat and fish. Large amounts of meat and fish would need to be consumed to obtain gram quantities of creatine, so supplementation is a practical alternative. Of the creatine in muscle, 60 – 70% are phosphorylated and the rest exists as its free form. Despite its ability to rephosphorylate ADP, its usefulness is limited to short-term, high-intensity exercise as it’s been shown that its effects may decrease as the length of time of the exercise increases.
Research
The following part of the article will include two summaries of research investigating the effect of oral creatine supplementation using creatine monohydrate, the most commonly used form of creatine. Research has consistently found that supplementation taken concurrently with resistance training leads to the greatest increases in strength, however responses to supplementation can vary from individual to individual.
Arciero et. al investigated the effects of creatine supplementation over a 4-week period in combination with resistance training. 20 g of creatine was initially taken per day for the first five days of the study, then tapered off to 10 g per day for the remainder of the study. “Loading” creatine supplementation, where larger amounts are taken within the first couple days of supplementation, has been found to cause the quickest increases in muscle creatine concentration; however, this step is not necessary because similar muscle creatine concentrations can be obtained over a longer period of time with smaller dosages.
The subjects were separated into three groups: creatine supplementation with resistance training (Cr-RT), creatine supplementation without resistance training (Cr), and placebo with resistance training (P-RT). The participants were tested for their 1RM, which is the maximum amount of weight that can be lifted with proper form for one repetition, in the bench press and leg press. Cr had strength increases of 8 and 16% in the bench press and leg press respectively, while Cr-RT saw maximal strength increases of 18 and 42%.
This was the first study to demonstrate that creatine supplementation with a well-designed resistance training program produced greater maximal strength increases than creatine alone. It should be noted that all groups, including P-RT, significantly increased their maximal strength, however Cr-RT had the greatest increases. The authors suggested that the results can be explained by previous research that found increases in resting creatine concentrations and rate at which phosphocreatine is resynthesized between sets following supplementation. These results are not unique, as Rawson and Volek have also found similar positive effects of creatine supplementation during weightlifting tasks in 17 of the 22 studies that they reviewed in 2003.
Individual responses to creatine supplementation have been examined by Syrotuik and Bell. The research used recreationally resistance-trained men who had no previous history of creatine supplementation and placed them into either a placebo or creatine supplement group. The creatine group supplemented with 0.3 g/kg/day. The researchers found that the supplemented group had the greatest increase in intramuscular creatine and phosphocreatine stores, while the unsupplemented group remained relatively unchanged. Participants that supplemented with creatine were able to be further categorized into three different groups – responders, quasi-responders, and non-responders – based on total intramuscular creatine and creatine phosphate stores following supplementation. In summary, it was found that participants in the study that had the lowest initial intramuscular phosphocreatine and creatine amounts and the largest percentage of muscle fibres involved in explosive movements had the greatest increases in creatine uptake.
Ethics of Supplementation
Some adjectives which have been used to describe creatine, such as “performance-enhancing” and “muscle-building”, have naturally produced discussion about its ethics and the possibility of its supplementation providing an unfair advantage. Some organizations have even made the argument that creatine supplementation would influence an athlete to experiment with other supplements or drugs, even going as far to place creatine in the same category as anabolic steroids and other banned substances.
It should be noted that the International Olympic Committee (IOC) has considered many arguments against its supplementation and stated that there was no need for its ban. The IOC stated that supplementation should be treated as any food because it can easily be found in meat and fish.
Further, creatine supplementation is not banned by any organization as of a 2007 review article in the Journal of the International Society of Sports Nutrition, but the National Collegiate Athletic Association (NCAA) does prohibit its distribution, along with other muscle-building products, to its athletes but does not ban its use independently.
Conclusion
As a final note, there has been no research indicating any short term or long term detriment associated with creatine supplementation. Both short and long term studies have found creatine supplementation to be safe when following recommended guidelines.
Creatine has been found to be a legal and safe dietary supplement that aids in athletic performance and strength development and its effects are maximized when taken in conjunction with resistance training.
References
DMAA in Dietary Supplements. U.S. Food and Drug Administration. http://www.fda.gov/Food/DietarySupplements/ProductsIngredients/ucm346576.htm (accessed Oct 17, 2016).
Stout, J.R.; Antonio, J.; Kalman, D. Overview of Creatine Metabolism. Essential of Creatine in Sports and Health. Humana Press: Totowa, N.J., 2008, pp 1-23.
Rowbottom, M. Drugs in sport: Creatine given all-clear by IOC. Independent [online], December 14, 1998. http://www.independent.co.uk/sport/drugs-in-sport-creatine-given-all-clear-by-ioc-1191609.html (accessed October 15, 2016).
East, D.B. Biochemical Pathways of Creatine and Creatine Phosphate. Honors Thesis. University of Tennessee, Knoxville, TN, 2002.
Clark, J. Creatine and phosphocreatine: A review of their use in exercise and sport. J Athl Train 1997, 32, 45-51 and references therein.
Cooper, R.; Naclerio, F.; Allgrove, J.; Jimenez, A. Creatine supplementation with specific view to exercise/sports performance: an update. J Int Soc Sports Nutr 2012, 9, 33- and references therein.
Volek, J.S.; Rawson, E.S. Scientific Basis and Practical Aspects of Creatine Supplementation for Athletes. Nutrition 2004, 20, 609-614 and references therein.
Volek, J.S.; Rawson, E.R. The effects of creatine supplementation and resistance training on muscle strength and weightlifting performance. J Strength Cond Res 2003, 17, 822-831.
Arciero, P.J.; Hannibal, N.S.; Nindl, B.C.; Gentile, C.L.; Hamed, J.; Vukovich, M.D. Comparison of creatine ingestion and resistance training on energy expenditure and limb blood flow. Metabolism, 2001, 50, 1429-1434.
Syrotuik, D.G.; Bell, G.J.; Burnham, R.; Sim, L.L.; Calvert, R.A.; MacLean, I.M. Absolute and relative strength performance following creatine monohydrate supplementation. J Strength Cond Res 2000, 14, 182-190.